
MEET LORA PARKS – I do silly. I do homeschool. I am a wife and Mom and I own a traveling photography business. I was ill for 2 decades from random illnesses all eventually pointing to Hyperparathyroidism. My Christmas gift in 2015 was my life. I had a successful surgery to remove a parathyroid adenoma at the Norman Parathyroid Center after already having a failed minimally invasive surgery elsewhere. Every day since has been a new adventure.
You can contact Lora via her Facebook page and Twitter @parkspix
HERE IS LORA’S STORY…..
LISTEN TO ME!!! PLEASE!!! LISTEN TO ME!!! WHY WON’T ANYONE LISTEN TO ME!!! THERE IS REALLY SOMETHING WRONG!!!! LISTEN!!!
YES! That’s really how i felt for years. Many, many, years. Although i actually don’t know for sure how many….and the further i get into recovery from my successful parathyroid adenoma surgery, the more i remember, the more i realize how long it really was.
Did it start in 1980 when i started getting ‘fainty’ if i didn’t eat every 3 hours? Was it in 1987 when i kept going in to the Dr. complaining that everything was making me ill and having them look at me and say i was young and ‘perfect’ and it COULD be just nervous stomach, anxiety…but really what did i have to be worried about, i was 20, right? Or was it years of feeling anxious over large crowds and loud noises, bright lights, no night driving? Or was it having to have back surgery to clean out exploded discs in my back for ‘no apparent reason’ in 1995? Was it in 2001 when i had to wear a mobile heart monitor because i was having extreme heart racing for ‘no reason’? Or was it when i started having numerous bouts with anemia for ‘no apparent reason’ in 2005 or the years of food sensitivities and asthma and heart murmors that are magically gone now? Or the years and years of infertility? What about the years of insomnia, exhaustion, and fogginess? Or the numerous mysterious trips to ER with vomiting and cramping and being told my appendix needed to come out STAT only to find out a few minutes later that everything was ‘fine’. Was it the years of the “guess which food will make you vomit” game…..I don’t even know any more! I do know that I have visited Urgent Cares/Emergency rooms in at least 5 states and British Columbia.
I have started to write down my story so many times. Anyone that has dealt with this disease can agree that when you get told over and over that you are ‘fine’ you start thinking it’s all in your head. Over the years i learned to just eat better, mostly….to choose which crowded activity i will or will not do, to drive vs. fly, but mostly i just learned to get by. I am a photographer and i try to push myself to get out on a daily basis and take my daughter to the parks, and just experience life with her. My life with this disease taught me to get creative and always pack crackers, Tums, kleenex, because we were traveling and always had to run to the restroom on the road, there were even times when i traveled with a rubbermaid tote under the seat of my car because really getting sick in the van while driving is an actual thing.
I was finally ‘diagnosed’ with a problem in 2012 by an RN who told me my calcium was 10.6. She made me promise to see an Endocrinologist and figure out what was going on. So i found one, saw he had a gorgeous website that stated that he did minimally invasive parathyroid surgery, he was local and i emailed his office immediately. The office staff was so friendly and helpful and had me send over my test results. My calcium was 10 at the time and as we were leaving for Canada for work right away they said it wasn’t ‘urgent’ and it could wait. I continued to struggle, both in Canada and Washington state, testing in both locations. If you look up Hyperparathyroidism symptoms, they are very random. But even the random ones i have had. Every.Single.One. I found the site parathyroid.com and learned so much. I learned that i was indeed ill, that it wasn’t in my head. That i needed surgery. But, surely there a local option…i hate hate hate to fly! No, i’m not afraid to fly, but i get so ill with all of the strange smells and noise and movement…can I fly? Well, unfortunately i decided i should try a local Dr. and ‘save’ myself time and money from going to Florida.
By 2015 I was so not myself. Not myself at all. I was having hand tremors, massive headaches, and my words were not coming out! My vomiting spells had gotten so bad that almost every food had the chance of setting me off. I had a huge attack with stabbing pains and vomiting tiny crystals, and I started calling Drs. again to find answers including internists and getting ultrasounds almost hoping they could find something else wrong and someone would be able to figure it out! Thankfully most of my friends and family were patient with me as I continued to get worse and worse, but still some days were ok and I could function. I got to the point of almost not driving because i was so ‘foggy’.
So, i contacted the surgeon in my local area, who performs minimally invasive parathyroidectomies, you know the one with the great website, the one that said he had all the experience….again and he said it was ‘time’. They set me up for countless more tests, including 24 hour urine catch, (EWWWWW) nuclear tests, etc. yay i was finally going to be done and better, right? The surgery day came. (April 2015)I went to the hospital in the am, met the staff, and woke up about 4 hours later by the Dr. who very nicely told me that they ‘couldn’t get it”. WTF? All of this for nothing? Yep. Not only could they not get to the adenoma, i had no memory of what had happened after surgery for the first 16 hours or so, and the meds that they had given me made me vomit almost constantly and have vertigo for almost 3 days straight. When i called the Dr. office they gave me a RX for nausea meds and I was told that this sometimes happens. I went in for my recheck after surgery and they told me that the hospital had run out of ‘blue dye’ and this would have been the other way they could have gotten to the adenoma. HUH?
Fast forward and i’m now feeling even worse than before surgery! When my brain finally clears enough to think and process, i went back to the parathyroid.com website and clicked on the area where it says, BECOME OUR PATIENT. I filled everything out. I knew there would be an even larger out of pocket cost because i let another surgeon touch me first…..i didn’t care. I knew that i had to fly to Florida……i didn’t care. I knew they would be saving my life.
When i got the first phone call from the ladies at the Norman Parathyroid Center, i was thrilled. I knew they had heard it all before, i knew that I didn’t need to explain anything to them, that they would get all of my medical records and make a plan. I patiently awaited the call from the man. (well, you know…i tried to be patient) When Dr. Norman called, i almost cried! It was really like getting a phone call from a long-lost friend. I knew that he was the answer. I knew that he could ‘fix’ me.
My husband and i flew in Tampa, stayed right downtown, walked everywhere. We also rented a car because we wanted to further explore. When we got to the hospital, we met everyone! It was amazing, so welcoming. They talked to me the entire way, and each Dr. stopped to say hi, and see if we understood everything, make sure we were all on the same ‘page’. Yes, since it was a second surgery I knew that the Drs. had to work with scar tissue, and it might take longer, or maybe they wouldn’t be able to help me but I also knew that this was my only chance. No surprises is huge when your brain is super messed up! My husband patiently waited for me and off we went…..
The surgery went great, I was told that there was almost no scar tissue and they were in and out and done in no time! I was handed a photo that says my trouble maker was testing at over 900 prior to removing it.I was so completely overwhelmed after I saw my picture of the adenoma ‘punk’ that tortured me for years that i was crying and asked to get my picture with Dr. Norman, which i posted to my work Instagram account for the entire world to see. We went back to the hotel after surgery, i took a little nap, and seriously, when i woke up it was like a switch was turned back on! I was ‘here’ again.
After resting and eating lunch, YAY, hungry! I asked my husband to take me to the beach! We drove over to Clear Water and walked and talked on the beach. The water was crystal clear, just perfect. We spent the next two days in Florida having long conversations, and I could follow along and not drift away! We walked and walked and I even danced at the winter celebration in downtown Tampa.
It has now been over 2 months since my surgery, i have almost no tired days…. i am sleeping, i’m hungry, and my hair is growing in! I have had no random pains, no kidney stones, no heart racing, no fogginess……every day is better than the next! I now know that my calcium should have been a flag to get more tests, not just to accept that 1. Maybe I just have a high count all the time…. or 2. That we should just have a ‘wait and see’ approach. I now know that I will do everything I possibly can to help people understand that it’s ok to ask for help, find someone to listen. It’s really hard to hear there is nothing wrong with you when you know there is. It is horrible to have to live with an illness that people don’t understand so they think you are making it up. My family and friends didn’t understand because I would go for long periods of time feeling ‘normal’, and able to do pretty much anything I wanted to do, and then I would have a spell for a few days and not able to do anything. The truth is, that I wanted to do EVERYTHING! And now I can. 😉
The first pic is as we are flying to Florida. (look at how exhausted I am!) The second, right after surgery with Dr. Norman (have I told you I love him???) and the third photo is the same day, with my husband, celebrating my new life!







 We know that often the first major obstacle for patients who have primary hyperparathyroid disease face is getting an accurate diagnosis in a timely manner.
We know that often the first major obstacle for patients who have primary hyperparathyroid disease face is getting an accurate diagnosis in a timely manner.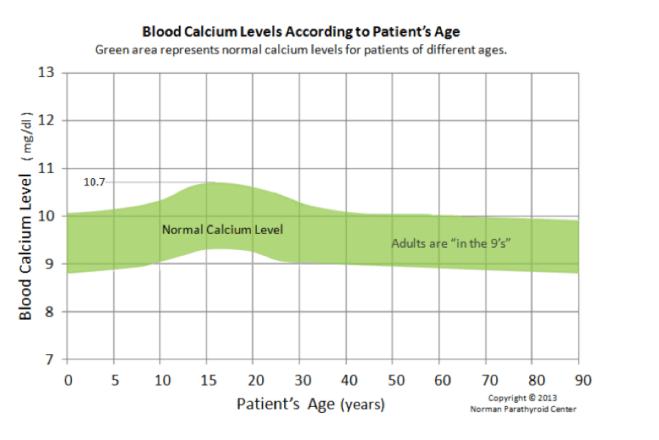








 This past week on a beautiful, sunny, blue-sky afternoon, with a view of the San Francisco Bay in the background, we held our bi-monthly Para Peeps meet-up at Chevy’s in Emeryville, CA. Our little group has now grown to 15 and we were please to have 8 of these members in attendance this time! At one point we all realized that this was our first time ever being surrounded by so many with “peep” scars. We laughed as we all pointed and showed off ours, noting that they are nearly invisible. For some of us years have passed since we had our surgeries, others months, while one member just got back from traveling across the country for surgery less than a week ago. She was in good spirits and was feeling energetic, happy to be moving forward towards improved health.
This past week on a beautiful, sunny, blue-sky afternoon, with a view of the San Francisco Bay in the background, we held our bi-monthly Para Peeps meet-up at Chevy’s in Emeryville, CA. Our little group has now grown to 15 and we were please to have 8 of these members in attendance this time! At one point we all realized that this was our first time ever being surrounded by so many with “peep” scars. We laughed as we all pointed and showed off ours, noting that they are nearly invisible. For some of us years have passed since we had our surgeries, others months, while one member just got back from traveling across the country for surgery less than a week ago. She was in good spirits and was feeling energetic, happy to be moving forward towards improved health.


 I used the
I used the 
 There are several issues that we would like to shed light on through this social media platform. Below are just a few examples of the issues we would like to raise awareness about by tweeting. We believe that our efforts would be far more effective with your help.
There are several issues that we would like to shed light on through this social media platform. Below are just a few examples of the issues we would like to raise awareness about by tweeting. We believe that our efforts would be far more effective with your help.